EMG-NCV is generally broken down into 2 parts.
 1. The NCV test wherein electrodes or wires are placed on specific parts of the body depending on what nerve to test. Then a small probe that stimulates the nerve is initiated in order to see how fast or how slow the nerve traveled from the point of stimulation up to the point where the wires are placed. Usually more than one nerve is tested and may require comparison with the other side.
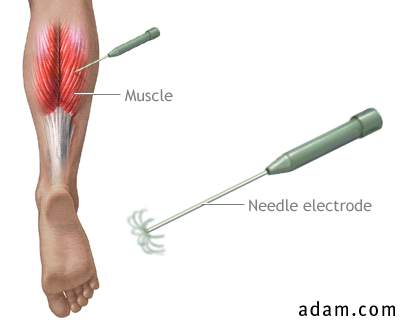
1. The NCV test wherein electrodes or wires are placed on specific parts of the body depending on what nerve to test. Then a small probe that stimulates the nerve is initiated in order to see how fast or how slow the nerve traveled from the point of stimulation up to the point where the wires are placed. Usually more than one nerve is tested and may require comparison with the other side.2. The EMG test is using a hairlike size needle that is attached to a computer. The needle is then inserted into the particular muscle that needs to be tested. Sort of an injection needle being inserted into your skin. The needle is then left there to see the electrical activity or any abnormalities that can be seen during the procedure. A youtube video by dsbgd011 shows this procedure found here.
Pictures as reference are taken from monarch diagnostic website.
The website link also explain this test.
Do you need one?
Usually this could be recommended if the nerve affected is the one coming out from the spine(back) and goes to the periphery (either to the hands or feet) called the peripheral nerve. If the nerve being tested is the spinal cord itself or the brain which is medically the central nervous system, then this test might not be beneficial.
So what specific conditions can EMG-NCV be recommended?
Back or neck pains that consider an impingement of the nerves, weakness of muscles of the upper and lower limbs that suspects a compromised peripheral nerve. Some of this are carpal tunnel syndromes, brachial plexus injuries or lumbar/cervical radiculopathies. EMG-NCV can also be recommended on some systemic conditions such as diabetic neuropathies or Guillane Barre syndromes. Facial nerve problems or trigeminal neuralgias are some conditions also that EMG-NCV can be used.
If an MRI or an imaging study is already done, would you still need this test? What is the difference?
Imaging studies usually will show the picture of the area where the suspected problem is but that is all it will tell the physician. EMG-NCV supplements that by telling the physician the function or electrical physiology of the suspected nerve/muscle. It can help the physician know if the problem is recent, an old one and how severe it is.
So if you need one, I hope this helps out in explaining the procedure.
